
Breakthrough Oral Drug Slashes ‘Remnant’ Cholesterol by 60%: What TLC‑2716 Could Mean for Heart Health
A New Way to Tackle ‘Remnant’ Cholesterol: What the TLC‑2716 Trial Really Means for Your Heart
If you’ve worked hard on your diet, taken your statin faithfully, and still worry about heart disease, you’re not alone. Many people discover that even with “good” LDL numbers, their blood can still carry a type of fat called remnant cholesterol that quietly raises the risk of heart attack and stroke. A new oral drug, TLC‑2716, has just shown the ability to cut these remnant particles by more than 60 percent in an early human trial, sparking cautious optimism among cardiologists and patients alike.
In this article, we’ll unpack what remnant cholesterol is, what the new ScienceAlert‑reported TLC‑2716 study actually found, how this fits into the latest heart‑health science as of early 2026, and—most importantly—what you can do right now to lower your own risk while researchers continue testing this promising treatment.
What Is ‘Remnant’ Cholesterol and Why Does It Matter?
Most of us learn about “good” HDL and “bad” LDL cholesterol. Remnant cholesterol is different. It’s the cholesterol carried inside triglyceride‑rich lipoproteins—mainly very‑low‑density lipoproteins (VLDL), intermediate‑density lipoproteins (IDL), and chylomicron remnants.
These remnant particles:
- Are rich in both cholesterol and triglycerides.
- Can penetrate the artery wall and deposit cholesterol, much like LDL.
- Are strongly linked with atherosclerosis, heart attack, and stroke, especially in people with diabetes, obesity, or metabolic syndrome.
“We’re realizing that remnant cholesterol is not just ‘background noise’ in the lipid profile—it’s a major causal factor in cardiovascular disease, especially when triglycerides run high.”
— Adapted from recent lipid research reviews in leading cardiology journals
In large genetic and observational studies published over the last decade, higher remnant cholesterol has been independently associated with more heart disease, even when LDL is well controlled. That’s why new drugs targeting remnant and triglyceride‑rich particles are attracting intense interest.
Inside the TLC‑2716 Trial: A New Oral Drug That Cuts Remnant Cholesterol by 60%+
According to a February 2026 report highlighted by ScienceAlert, an early‑phase clinical trial of TLC‑2716—an experimental oral lipid‑lowering compound—showed substantial reductions in blood fats strongly linked to heart disease, including remnant cholesterol.

While the full peer‑reviewed paper is still emerging, publicly reported highlights from this early trial include:
- Population: Adults with elevated triglycerides and remnant cholesterol, many already at higher cardiovascular risk.
- Form: Oral medication, taken by mouth (unlike some injectable lipid therapies).
- Effect on triglycerides: Average reductions of more than 60%.
- Effect on remnant cholesterol: Similar magnitude of reduction—over 60% in many participants.
- Tolerability: Early data suggest the drug was generally well tolerated over the short trial duration.
These results are exciting because they suggest we may soon have a powerful oral option specifically targeting the triglyceride‑rich particles that drive remnant cholesterol, beyond what statins alone can do.
How Might TLC‑2716 Work to Lower Remnant Cholesterol?
The exact mechanism of TLC‑2716 is still being explored, but based on current disclosures and comparable agents, researchers suspect that it targets key steps in the production or clearance of triglyceride‑rich lipoproteins in the liver and bloodstream.
- Less production of triglyceride‑rich particles The liver may release fewer VLDL particles into the blood, meaning fewer building blocks for remnant cholesterol.
- Faster clearance from the bloodstream TLC‑2716 may enhance the body’s ability to break down and remove triglyceride‑rich particles before they lodge in artery walls.
- Downstream impact on artery health With fewer remnant particles, there is potentially less inflammatory and cholesterol burden inside arteries.

Similar classes of triglyceride‑focused drugs (such as those targeting apoC‑III or ANGPTL3) have already shown that selectively lowering triglyceride‑rich lipoproteins can dramatically shift remnant cholesterol levels. TLC‑2716 appears to be part of this new wave, but in an oral tablet form, which could be more convenient for many patients if proven safe and effective.
What We Know So Far—and What We Don’t Yet Know
Early TLC‑2716 data are promising, but it’s important to keep expectations grounded in what science can currently support.
Strengths of the current evidence
- Substantial, rapid reductions in triglycerides and remnant cholesterol (>60% in many participants).
- Oral dosing, which could improve adherence compared with injectable therapies.
- Biological plausibility based on strong prior evidence linking remnant cholesterol with cardiovascular risk.
Key unanswered questions
- Will TLC‑2716 actually reduce heart attacks, strokes, and death in large, long‑term clinical trials?
- How will it compare with, or add to, existing therapies like statins, fibrates, omega‑3s, PCSK9 inhibitors, or newer agents targeting apoC‑III and ANGPTL3?
- Are there rare or long‑term side effects that shorter studies cannot detect?
- Which patients will benefit most—those with diabetes, severe hypertriglyceridemia, familial disorders, or broader high‑risk groups?
“Lowering a risk marker is encouraging, but cardiologists ultimately care about events—fewer heart attacks, fewer strokes, and longer, healthier lives. That’s what the next wave of TLC‑2716 studies has to show.”
— Perspective consistent with current cardiovascular outcomes research
A Real‑World Scenario: When LDL Looks Good but Risk Stays High
Consider a typical patient story—details changed to protect privacy, but similar to what many clinicians see.
“Maria,” a 58‑year‑old woman with type 2 diabetes, had worked hard on her health. Her LDL cholesterol was well controlled on a statin, her blood pressure was decent, and she walked most evenings. Yet her triglycerides stubbornly hovered around 300 mg/dL, and her doctor calculated that her remnant cholesterol remained high.
Despite “good” LDL, Maria’s cardiologist explained that those triglyceride‑rich remnants still increased her risk of heart attack. They optimized her diabetes care, adjusted her diet to reduce refined carbohydrates, and added high‑dose prescription omega‑3s. Her triglycerides improved but didn’t normalize.
For patients like Maria, drugs such as TLC‑2716 could—if eventually approved—offer a targeted way to push triglycerides and remnant cholesterol much lower. For now, she and her care team focus on the proven tools already available, while keeping an eye on emerging treatments through reputable medical updates.
What You Can Do Now to Lower Remnant Cholesterol and Protect Your Heart
While we wait for more data on TLC‑2716, there is a lot you can do—starting today—to reduce triglycerides, remnant cholesterol, and overall cardiovascular risk. None of these steps are magic, but together they can make a meaningful difference.

1. Focus on triglyceride‑smart nutrition
- Cut sugary drinks and refined carbs (sodas, sweets, white bread, pastries); these rapidly drive up triglycerides.
- Choose whole, minimally processed carbs like oats, beans, lentils, and whole grains.
- Favor healthy fats (olive oil, nuts, seeds, avocado) over trans fats and deep‑fried foods.
- Limit alcohol, especially if your triglycerides are high—alcohol can sharply raise them in some people.
- Include fatty fish (salmon, sardines, mackerel) 1–2 times per week for natural omega‑3 fats.
2. Move your body most days
Regular physical activity helps lower triglycerides, raise HDL, and improve insulin sensitivity.
- Aim for at least 150 minutes per week of moderate‑intensity activity (like brisk walking) or as advised by your clinician.
- Add 2 days of resistance training (bands, weights, body‑weight exercises) to support metabolism.
- If you’re starting from zero, begin with 5–10 minutes a day and increase gradually.
3. Optimize blood sugar and weight
Elevated blood sugar and excess abdominal fat are tightly linked to higher triglycerides and remnant cholesterol.
- Work with your clinician to keep your HbA1c in the target range if you have diabetes or prediabetes.
- Even a 5–10% weight loss can noticeably improve triglyceride levels for many people.
4. Use proven medications consistently
Before adding new drugs, it’s essential to make the most of therapies with strong outcome data.
- Statins remain the cornerstone for LDL and overall cardiovascular risk reduction.
- Your clinician may consider fibrates, prescription omega‑3s, or other agents if your triglycerides are very high.
- For very high‑risk patients, PCSK9 inhibitors or other advanced therapies may be appropriate.
- Whatever your regimen, taking medications as prescribed often matters more than which brand you’re on.
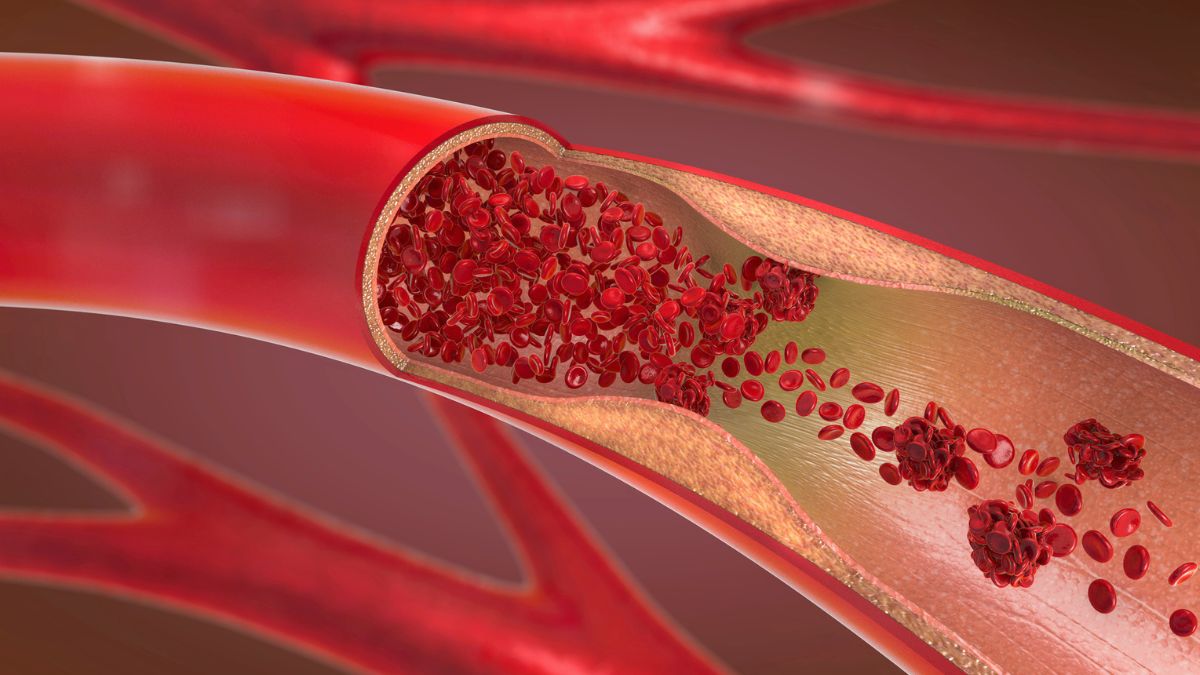
Visualizing the Impact: Arteries Before and After Remnant Cholesterol Reduction
While we can’t see your arteries changing in real time, imaging studies show that aggressive lipid‑lowering—especially when started early—can slow, and sometimes modestly reverse, plaque buildup.


We still need direct outcomes data on TLC‑2716, but existing research strongly supports the idea that lowering atherogenic lipoproteins (LDL, remnant cholesterol) is a key part of preventing heart attacks and strokes.
How to Talk With Your Doctor About Remnant Cholesterol and New Treatments
If the TLC‑2716 news caught your attention, that’s a signal you care about your heart health. The next step is having a clear, collaborative conversation with your clinician.
Questions you might ask
- “Do my triglyceride and remnant cholesterol levels put me at higher risk?”
- “Are there changes in my diet, activity, or medications that could help lower them?”
- “Am I already on optimal, evidence‑based therapy for my overall cardiovascular risk?”
- “Are there any clinical trials for triglyceride‑lowering or remnant‑cholesterol drugs that might be appropriate for me?”
Many cardiology centers participate in research on new lipid‑lowering drugs. If you’re interested, your doctor can help you weigh the potential benefits and risks of trial participation versus continuing with standard care alone.
Trusted Resources to Learn More
For deeper dives into remnant cholesterol, triglycerides, and emerging therapies like TLC‑2716, consider:
- American Heart Association – Patient‑friendly information on cholesterol, triglycerides, and heart disease prevention.
- American College of Cardiology – Professional guidelines and updates on lipid management and cardiovascular risk.
- National Heart, Lung, and Blood Institute (NHLBI) – Evidence‑based information on high blood cholesterol and treatment options.
- Peer‑reviewed reviews on remnant cholesterol and cardiovascular risk in journals like Circulation, European Heart Journal, and Journal of the American College of Cardiology.
Looking Ahead: Hope, Caution, and Action You Can Take Today
TLC‑2716’s ability to cut remnant cholesterol by more than 60 percent in an early trial is a meaningful scientific step forward. It suggests we may soon have a potent oral tool aimed directly at a long‑under‑recognized driver of heart disease. At the same time, it’s too early to say whether this drug will become part of routine care, or exactly who will benefit most.
While researchers continue the careful work of larger, long‑term trials, you are far from powerless. By combining:
- Triglyceride‑smart nutrition,
- Regular physical activity,
- Thoughtful management of weight, blood sugar, and blood pressure, and
- Consistent use of proven medications under medical guidance,
you can significantly reduce your risk of heart attack and stroke—starting now.
Your next step: choose one small, specific action you can take this week—booking a check‑up, adding a 10‑minute walk after dinner, or swapping a sugary drink for water—and commit to it. Real heart protection is built from many small, sustainable steps, not just the next breakthrough drug.
